Earth, Inc. Shareholder Report: Human Capital
| Topics: |
HUMAN CAPITAL: Human capital includes (but is not limited to) the health, physical ability, intelligence, knowledge, and all the other attributes of individual people that allow each of us to function in a complex society. Human Capital also captures human dimensions that contribute to well-being such as education and happiness.
Contents
- 1 Report on Human Capital: Life Expectancy and Health Expenditures
- 1.1 Introduction: In this report, human capital is not just a measurement of the physical labor of humans and the know-how stored in their brains, that might contribute to industrial production. We define Human Capital as a measure of all the human dimensions that contribute to well being. A variety of indicators could be used including life expectancy at birth, literacy or illiteracy rates, infant mortality rates, health expenditure, and education expenditure. In this section we will look at life expectancy at birth as a "stock" of years, and per capita health expenditure (in current United States dollars) as a flow of resources that adds or detracts from life expectancy. Data for life expectancy was obtained from the World Bank for the years 1990 and 2000. Data for per capita health expenditure was collected for the period 1990-1998, also from the World Bank. In analyzing this data, it was noted that health expenditure data were not available for any country in the Former Soviet Union until 1992 and most countries in the region (Earth, Inc. Shareholder Report: Human Capital) until 1994.
- 1.2 Stocks: Life Expectancy
- 1.3 Flows: Health Expenditures
- 1.4 Case Study: Botswana
- 2 Further Reading
Report on Human Capital: Life Expectancy and Health Expenditures
Stocks: Life Expectancy
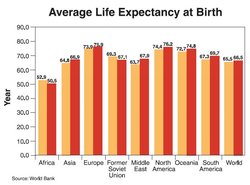 Average life expectancy at birth. (Source: World Bank)
Average life expectancy at birth. (Source: World Bank) Worldwide average life expectancy increased slightly (1 year) from 65.5 years in 1990 to 66.5 years in 2000. Regionally, all areas except the former Soviet Union and Africa showed an increase. The Middle East experienced the largest gain of 4.2 years. In the Former Soviet Union and Africa, life expectancy decreased by 2.1 years and 2.4 years respectively.
In the Former Soviet Union, this decline is likely attributed to a variety of factors related to the collapse of the Soviet Union in 1990 and its republics declaring independence. The transition from centralized governance to independent states was not necessarily a smooth process and a decline in basic services was likely. According to United Nations Development Programme (UNDP),
“The political process of the breaking up of the Soviet Union has been remarkably peaceful, but also resulted in a "state desertion", with a governance vacuum still unresolved… When transition becomes only a partial process, primarily benefiting the young, the dynamic, the mobile, the connected, and leaving behind the vulnerable, then the surge in poverty, already so visible, will destabilize societies and reverse whatever this new economic growth is capable of.” (UNDP/RBEC, 1999)
Additionally, the decline may be a result of problems with the data. Because the Soviet Union and its republics were undergoing major changes in 1990, the data collected during that transition period is likely to be less accurate than more recent data. As noted above, health expenditure data was not even available during the early 1990s. In acknowledging of the need for better data in this region, the UNDP Regional Bureau for Europe and the Commonwealth of Independent States (REBC), responded by developing a program for Human Development Statistics and Reporting in the early 1990s. The goal of this program is to meet the "urgent need to develop, collect, analyze and publish social and demographic statistics" (UNDP/RBEC), and it began publishing National Human Development Reports in 1995.
Each year the report publishes the latest trends in the quality of people's lives as measured by economic factors, including per capita GNP, social and human factors, such as health and education (UNDP/ RBEC). Therefore, post-1985 data probably more accurately depicts trends in this region.
Decline in life expectancy in Africa is primarily attributed to the HIV/AIDS epidemic on the continent. Worldwide outbreaks began in the mid-1980s and between 1990 and 2000 the disease reached epidemic levels on the African continent. Africa continues to suffer the effects of HIV/AIDS much more than the rest of the world. Africa is home to 70% of the adults and 80% of the children living with HIV/AIDS in the world (AVERT). The impacts of the epidemic are both human and socioeconomic. The challenge facing Africa is not only in "sustaining and expanding prevention successes, but in providing adequate treatment, care and support to the millions of people living with HIV/AIDS or orphaned by the epidemic" (UNAIDS, 2002).
Flows: Health Expenditures
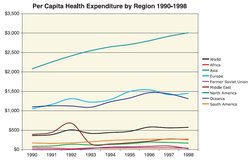 Per capita health expenditure by region, 1990-1998. (Source: Authors)
Per capita health expenditure by region, 1990-1998. (Source: Authors) Expenditure on health care varies tremendously around the world (Figure 2). For example, in 1998 the United States spent $3,010.39 on each of its citizens while Ethiopia expended only $4 per person. In 1998 an average of $597.29 was spent on each world citizen. This represents about a 50 percent increase per capita health care expenditure worldwide above the 1990 average of $373.50.
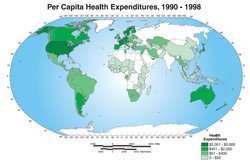 Per capita health expenditure, 1990-1998. (Source: Authors)
Per capita health expenditure, 1990-1998. (Source: Authors) Regions seem to cluster in three groups regarding per capita health expenditure: less than $500, between $1,000 and $2,000, and greater than $2,000. The [[region]s] containing "developing" countries, including Africa, Asia, Former Soviet Union, South America, and the Middle East generally comprise the less than $500 category. Oceania and Europe are in the second category with per capita health spending generally in the $1,100 to $1,500 range. North America is the lone region in the final category. It is important to note that in some regions one or two countries dominate the regional averages. In Oceania for example, New Zealand ($1133) and Australian ($1714 per capita in 1998) expenditures shape the regional average and make it appear as though the region has adequate resources for healthcare. However, the other two countries in the region for which 1998 data is available, Fiji and Papua New Guinea, have very low expenditures – $86 and $25 respectively. Canada and the United States' high expenditures similarly mask Mexico's low expenditure in the regional averages. Mexico should be among the countries that spend under $500 per capita on health care.
Case Study: Botswana
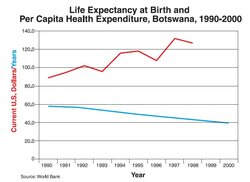 Life expectancy at birth and per capita health expenditure in Botswana, 1990-2000. (Source: World Bank)
Life expectancy at birth and per capita health expenditure in Botswana, 1990-2000. (Source: World Bank) Botswana has a relatively high per capita health expenditure compared to other countries in Africa. Per capita spending ranged from $89 in 1990 to $132 in 1997. This is well above the African average of $17.76 in 1993 and $44.70 in 1996. Despite this, Botswana experienced the world's most serious life expectancy decline, falling from 56.8 years in 1990 to 39.0 years in 2000. This decline can be attributed to the HIV/AIDS epidemic occurring on the African continent. Due to this epidemic, life expectancy at birth has been reduced to 39 years since the first reported case in 1985. The United States Agency for International Development (USAID, 2002) predicted that life expectancy would have been 72 years, if it were not for AIDS. While 19 percent of the general population has HIV/AIDS, the prevalence rates vary by age group. HIV/AIDS prevalence rate for those ages 15-49 is 39 percent, the highest in the world (Fredriksson & Kanabus). For individuals 15 years old and younger the rate of HIV/AIDS is less than 2 percent, but 58.1% (males) and 41.9% (female) of infant deaths are due to HIV/AIDS (UNDP Botswana).
This example illustrates that rising government health expenditures do not necessarily lead to improved life expectancy for all its citizens, as reflected in life expectancy. The (UNDP) states:
“Unlike in many other developing countries, in Botswana, financial resources have never been the most critical constraint on the design and implementation of a comprehensive and coherent HIV and AIDS programme. Yet, in 1998, 13 years since the first case of HIV and AIDS was reported, there was no semblance of a coherent government, let alone nation-wide, response to the epidemic.”
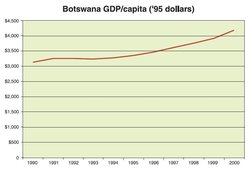 Botswana GDP per capita (1995 dollars). (Source: Authors)
Botswana GDP per capita (1995 dollars). (Source: Authors) Additionally, money invested to fight the epidemic had a low impact because:
“The volume of public resources allocated to its containment betrayed limited appreciation of the implications of HIV and AIDS for the economy, society, households and individuals. Policy and programme responses were thus severely hamstrung by excessive focus on government, especially the Ministry of Health, to the exclusion of other actors. (UNDP)
During the period when life expectancy declined by nearly 18 years, Botswana’s real GDP per capita was rising by nearly 34%. This was not due to a reduction in population (Population growth rate), because despite the decline in life expectancy, the overall population of the country was growing due to a high birth rate. Greater economic wealth per person was produced in 2000 than in 1990, but this had no impact on life expectancy, and as previously explained, money was not the limiting factor. This demonstrates how ludicrous it is to use GDP as a measure of human wellbeing.
 (Source: Authors)
(Source: Authors) However, there is hope for the region. Botswana is politically stable and has enjoyed a period of unbroken peace since 1966. Additionally, it has a steady and relatively lucrative income as a result of its diamond mines. The government is recognizing that its resources were not being targeted correctly, limiting its ability to contain the HIV/AIDS epidemic plaguing the country. The most recent response effort (1997-2002) was expanded to include education, prevention and comprehensive care including the provision of antiretroviral treatment and inclusion of many previously excluded stakeholders, such as youth and pregnant women. The overall aim is "not only of reducing HIV infection and transmission, but also reducing the impact of HIV and AIDS at all levels of society" (AVERT).
This report only touched on two aspects of human capital, life expectancy and health expenditure. In further investigating this relationship for the Former Soviet Union region and for Botswana, it was clear a multitude of factors impact both the amount of resources devoted to healthcare and life expectancy. These cases illustrate that government stability, equality, the HIV/AIDS epidemic, the manner in which government finances are allocated, the types of health-related programs the government supports, and many other factors are influential for human capital.
Further Reading
- AVERT. Aids in Africa Website. Retrieved May 6, 2003 at http://www.avert.org/aafrica.htm
- Costanza, R. (2001). Visions, Values, Valuation, and the Need for Ecological Economics. BioScience. 51(6), 459-468.
- Fredriksson, J. & Kanabus, A. HIV & AIDS in Botswana. Retrieved May 6, 2003 at http://www.avert.org/aidsbotswana.htm
- United Nations Development Programme (UNDP). Moving Upstream and Engaging Governments in Strategic Policy Advocacy: The Case of UNDP Botswana's HIV & AIDS Programme. Retrieved May 5, 2003 from http://www.undp.org/hiv/botswana.pdf
- United Nations Development Programme (UNDP) Botswana. HIV/AIDS Programme Website. Retrieved May 5, 2003 from http://www.unbotswana.org.bw/undp/hivaids.html
- United Nations Development Programme Regional Bureau for Europe and the CIS
- (UNDP/RBEC). (1999). Human Development Report For Central and Eastern Europe and the CIS. (Serial No. E.99.III.B.6). Bratislava, Slovakia.
- United Nations Development Programme Regional Bureau for Europe and the CIS
- (UNDP/RBEC). Human Development Statistics and Reporting Website. Retrieved May 6, 2003 from http://www.undp.org/rbec/programmes/
- United Nations Programme on AIDS (UNAIDS) (2002) Epidemiological Fact Sheets on HIV/AIDS and Sexually Transmitted Infections: Botswana, 2002 Update. Retrieved May 6, 2003 at http://www.unaids.org/worldaidsday/2002/press/index.html#facts
- United States Agency for International Development (USAID) (2002) Life Expectancy will drop worldwide due to AIDS, Press Release, July 8.
| This is a chapter from Earth, Inc. Shareholder Report (e-book). Previous: Built Capital|Table of Contents|Next: Social Capital |